Recently, a State Police agency in the Southwest identified a troubling trend: officers leaving the agency due to PTSD and related medical disability claims. These officers had previously served in the military and had experienced combat, including witnessing comrades killed in battle or by roadside bombs. However, the agency discovered that PTSD was linked not solely to military experiences, but also to the distressing and tragic fatal accidents officers responded to on state freeways.
Law enforcement officers face occupational challenges that are unique when compared to most professions. Regular exposure to traumatic and critical incidents is a reality for police officers, and this repeated exposure can lead to serious emotional health issues, including post-traumatic stress disorder (PTSD). The impact of trauma varies depending on whether officers directly experience a traumatic event, witness it in person, or learn that a close friend or family member has been involved in a life-threatening incident. But the cumulative trauma faced in law enforcement makes it nearly impossible for officers to avoid some degree of emotional impact over the course of their careers.
Unfortunately, stigma around seeking help persists, with many officers fearing they will be labeled as weak or emotionally unstable if they reach out for support. This reluctance to seek help ultimately harms both the individual officer and the department.
Case study: Albuquerque Police Department
The Albuquerque Police Department (APD) recently experienced the tragic loss of an officer to suicide. This officer, who was in his late 40s, had served in the military before joining APD and worked with the department for approximately three years. Unbeknownst to colleagues, he was receiving treatment for PTSD at the Veterans Affairs Hospital and was prescribed ketamine for treatment-resistant depression. Although officers are required to report any prescribed medications, no one was aware of his condition or the ketamine treatments. The officer was withdrawn and kept his personal struggles private.
Ultimately, the officer suffered a breakdown resulting in a domestic violence incident, during which he assaulted and threatened his wife and daughter. The situation escalated to felony warrants and a standoff at his residence, where he set fires, shot the family dog and took his own life. This case underscores the devastating consequences of unaddressed trauma and untreated mental health conditions among law enforcement personnel.
Barriers to seeking help
Despite the availability of multiple support options — including a peer support program, police chaplains, a department psychologist and an employee assistance program — many officers hesitate to seek help because of the perceived stigma. Concerns about being viewed as weak or unstable prevent some from accessing available resources. Officers may be reluctant to report colleagues who are struggling, fearing they will be labeled as “snitches.” Department leadership must strive to dismantle these barriers and emphasize that reporting concerns is an act of care, not betrayal.
Understanding PTSD and related conditions
PTSD often manifests after exposure to traumatic events involving actual or threatened death, serious injury or sexual violation. The exposure may occur through direct experience, witnessing the incident, or learning that a close friend or family member was involved in such an event, violent or accidental. In addition to PTSD, officers may experience vicarious trauma, compassion fatigue and burnout — conditions that are closely related to the demands and stresses of police work.
There are several symptoms associated with PTSD. These include:
- Avoiding thinking about or talking about the trauma
- Avoiding activities, locations or individuals that will cause recollection of the trauma
- Diminished interest in former activities
- Detachment or avoidance of others
- Personality changes
- Sense of hopelessness
- Sleep disorders
- Irritability and anger
- Inability to focus or concentrate
- Hypervigilance with exaggerated startle response
- Flashbacks and nightmares
Some PTSD triggers include “anniversary” dates associated with the trauma. Triggers can include sounds, like helicopters, gunshots or fireworks. Other triggers can be smells like fire or jet fuel, or rotten garbage that reminds the person of the smell of dead bodies.
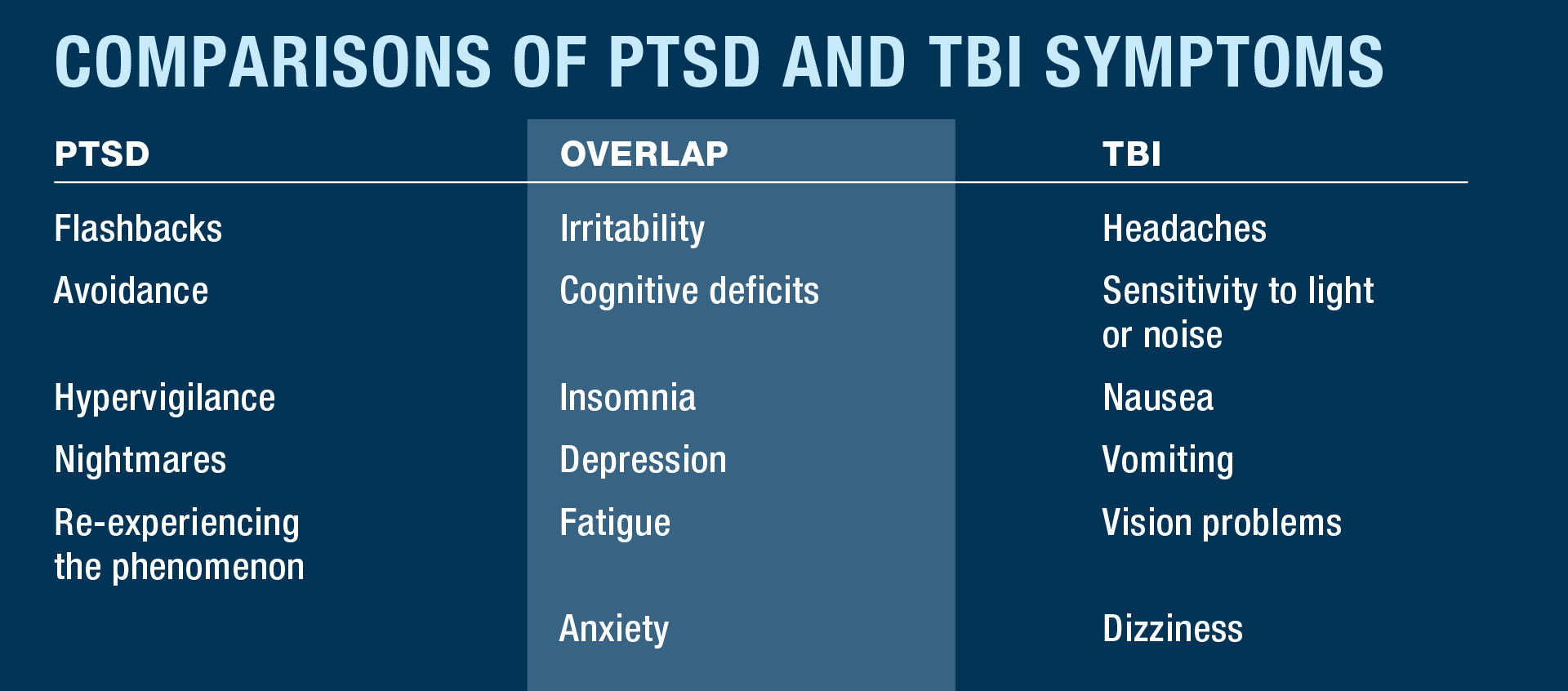
Recently, studies have revealed that the signs of a concussion or a traumatic brain injury overlap with those of a PTSD.
A comprehensive medical exam following a head injury should include a CT scan. Persistent post-concussive symptoms can exacerbate personality and behavioral issues, leading to serious consequences, including suicidal ideations. Studies have shown that prior blows to the head from contact sports or exposure to gunfire or flashbangs may cause some brain damage over the years and can lead to an early death if not detected. Many professional sports now follow a concussion protocol that requires a medical examination before returning to play again. The same protocol should apply when a police officer suffers a head injury during a fight or a serious car accident.
Signs of depression
Police officers are not immune to depression. Depression is triggered by a complex mix of factors, including stressful life events (trauma, loss, financial issues), genetics (family history), brain chemistry imbalances (neurotransmitters), personality traits (pessimism, low self-esteem), other medical conditions (chronic illness, sleep disorders), substance misuse (alcohol/drugs) and major life changes, creating a downward spiral of symptoms.
Common symptoms include:
- Lack of appetite or overeating
- Insomnia or hypersomnia
- Fatigue
- Low self-esteem
- Poor concentration, difficulty making decisions
- Feelings of hopelessness, worthlessness or helplessness
- Diminished interest or pleasure in activities
- Weight loss or gain
- Recurrent thoughts of death
- Crying easily
Officers exhibiting these symptoms should be referred to a professional therapist. They should be placed on administrative or medical leave until they are cleared for duty after a psychological evaluation. The department’s administrators will make the final decision on whether the officer should be released to full duty and should be advised of any medications prescribed for the officer.
Vicarious trauma and compassion fatigue
Vicarious trauma is the emotional residue or strain of exposure to those suffering from the consequences of traumatic events. Compassion fatigue can occur due to exposure to one incident or due to a cumulative level of trauma.
Some signs and symptoms of compassion fatigue can be exhaustion, insomnia, headaches and lowered resistance to illness. They can suffer from hypochondria and physical ailments. Officers can exhibit anger, irritability, and impaired judgment and decision-making, both on and off the job. They can develop relationship issues with fellow officers or family members. They will often lack a sense of enjoyment and have low job satisfaction. Some develop heightened anxiety and irrational fears. They can be cynical, hypersensitive and resentful and feel helplessness and hopelessness.
Sometimes homicide or child abuse detectives investigate horrific cases leading to compassion fatigue. To prevent this, departments should schedule “mental health checkup” visits with the department psychologist.
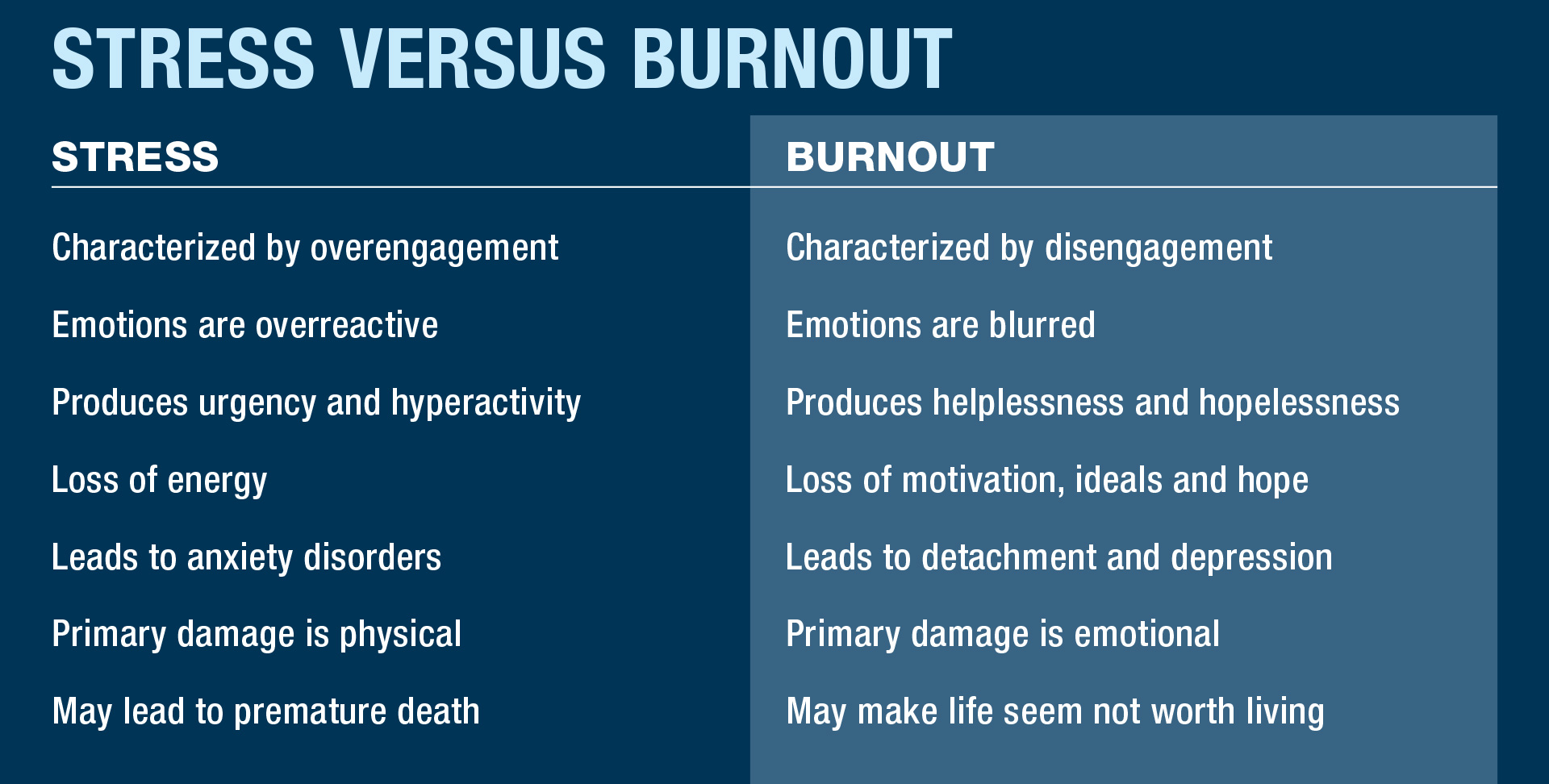
Understanding stress and burnout
Officers often complain about being stressed or burnt out. There are several work-related causes to both these conditions. Officers sometimes feel as if they have little or no control over their work. This occurs when there is lack of recognition or reward for good work. Sometimes there are unclear or overly demanding job expectations. Some officers feel that the job is monotonous or unchallenging.
One’s lifestyle can lead to burnout. Officers sometimes work too much, without any time for relaxation. They take on off-duty jobs or overtime assignments. They can be high achievers, with Type A personalities. They often lack quality sleep. Some officers lack close supporting relationships.
The physical signs and symptoms of burnout are feeling fatigued and frequently sick. There may be changes in appetite, frequent headaches, back pain and muscle aches.
Emotional signs and symptoms include a sense of failure, feeling helpless and defeated. There is a loss of motivation, and the officers are cynical, with a negative outlook. They may lack satisfaction or sense of accomplishment. Some behavioral signs include withdrawing from responsibilities, isolation, procrastination, tardiness and taking out their frustrations on others.
Officers should know their backgrounds and triggers. They should understand the signs and symptoms of PTSD, depression, suicide and vicarious trauma and use proper coping mechanisms. They need to understand and accept what is and isn’t in their control and take advantage of available resources.
Law enforcement crisis lines like CopLine are manned by retired officers 24/7 and are strictly confidential. If you or someone you know is struggling, please have them reach out to CopLine at (800) 267-5463, and/or seek professional help.
Mike Geier
As seen in the April 2026 issue of American Police Beat magazine.
Don’t miss out on another issue today! Click below: